
The ICL — clear vision with a lens inside the eye.
The ICL (implantable contact lens) is an additional lens placed inside the eye while keeping your own lens. It corrects short-sightedness, long-sightedness and astigmatism, tissue-sparing, without removing corneal tissue, and in principle removable again. For many eyes it is a full option for life without glasses, across a broad range of refractive errors, from lower to very high values. Whether it suits you is something we clarify together.
What is the ICL?
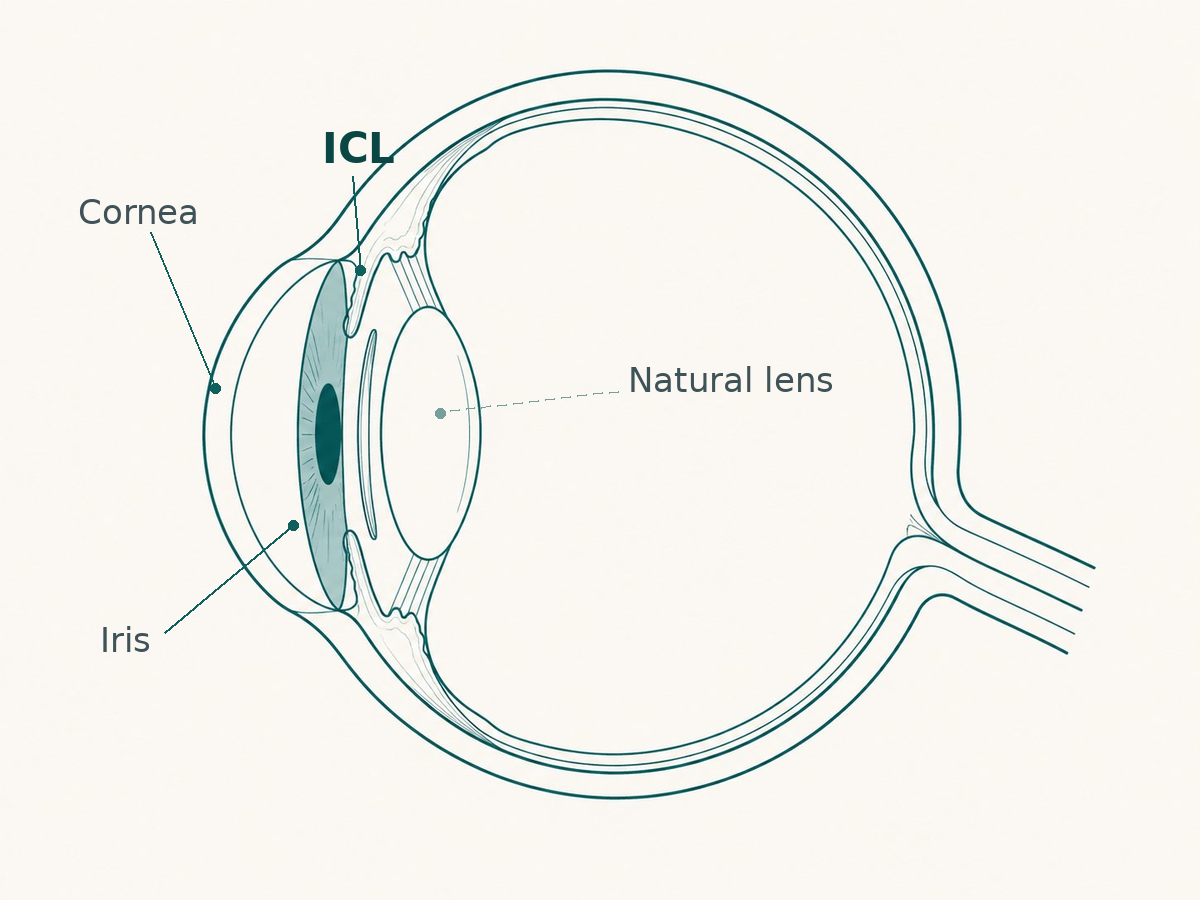
The ICL is placed into the eye in a single procedure and stays there permanently, behind the iris and in front of your own lens. Your natural lens is preserved and keeps working; the ICL complements it, much like a contact lens, only inside the eye rather than on its surface.
Not a last resort — an option in its own right
For a long time the focus was on very high short-sightedness or on eyes whose cornea isn't suited to laser, and there the ICL remains strong. Meanwhile the evidence has broadened: the ICL is increasingly considered an option in its own right at lower values too, not just a fallback. Because it removes no corneal tissue and does not stress the ocular surface the way a laser does, it can, depending on the eye, even be the more natural choice.
Research on the ICL
The ICL is not only a treatment for me, but a research topic. Among other things, I developed and peer-review-published two of my own formulas for calculating the power of these lenses: the Linz-Homburg-Castrop formula for the ICL (J Cataract Refract Surg, 2023) and the LION formula for ICL and IPCL (Am J Ophthalmol, 2024). An overview of my work on the ICL and phakic lenses is available on PubMed.
A lens in the eye — can you feel it?
One of the most common questions, and a fair one. The answer is clear: no. The ICL sits protected behind the iris and in front of your own lens. You don't feel it in everyday life, and it can't be seen from the outside.
How safe is the material?
The material of modern intraocular lenses has been in clinical use since the very beginnings of the intraocular lens, since Sir Harold Ridley implanted the first artificial lens. It is considered exceptionally well tolerated. Worldwide, and especially in Asian countries, ICLs are implanted in very large numbers. From this there is a broad body of data, grown over many years, on the safety and tolerability of the material, without any accumulation of problems attributable to the material itself.
Who is the ICL right for — and who not?
Whether the ICL is an option for you depends among other things on your refractive values, the depth of the anterior chamber inside the eye and the cornea's endothelial cell count, things a careful pre-examination clarifies. As with any procedure inside the eye, we weigh the benefit and the effort individually. Should the ICL not be the best solution for you, I will of course tell you so in our conversation and discuss the alternatives with you.
Laser or lens? Corneal laser and the ICL solve the same task in two ways, one at the cornea, the other with a lens inside the eye. Which one fits depends on your cornea, your refractive error and your daily life.
Is the ICL right for me?
That is decided by your eye and your visual priorities, not by a blanket rule. In consultation we clarify your values, your suitability and whether the ICL, or another path, makes sense for you.
Request a consultationGeneral information, it does not replace individual medical advice. Please do not include sensitive health data in your email.